
The biggest documentation risks in psychiatry billing right now center on 4 areas: telehealth modifier errors, missing time documentation, inadequate medical necessity language, and 42 CFR Part 2 consent gaps. Each of these gaps can cause claim denials.
Psychiatry billing has become more documentation-sensitive because payers now use AI-powered claim review systems that automatically detect:
- modifier mismatches,
- missing time records,
- repetitive psychotherapy notes,
- and unsupported treatment documentation.
As highlighted by Advanced Data Systems Corporation in its 2026 behavioral health analysis,
“Behavioral health billing is uniquely complex. Generic medical billing processes often fail to capture the nuances of psychiatry and substance abuse claims.”
A single documentation gap can now trigger payment delays or audit review much faster than before. The key issue now is to identify which documentation gaps are already putting your claims at risk.
Why Psychiatry Billing Documentation Fails More Than Other Specialties?
Several structural changes are making psychiatry billing more vulnerable in 2026.
Subjective Clinical Progress Needs Strong Documentation
Psychiatric treatment mostly focuses on emotional regulation and neuro-behavioral stabilization. These conditions are clinically meaningful, but it is difficult to translate these into payer-supported language.
Statements such as:
“Patient feels somewhat better”
or
“Discussed stressors and coping strategies”
usually do not establish medical necessity on their own. Payers expect that the psychiatric notes should clearly connect:
symptoms → diagnosis → treatment rationale → specific therapeutic intervention
in a more structured and defensible way.
Payers now expect psychiatric notes to connect symptoms, diagnosis, treatment rationale, and therapeutic intervention in a much more structured way.
Telehealth Billing Rules Became More Complex
Behavioral health uses telehealth the most in the United States. But the telehealth rules that continued into 2026 have stricter documentation requirements.
Practices must now correctly document:
- telehealth consent
- patient location
- provider location
- session modality
- correct modifiers
- accurate place-of-service coding.
Even small modifier mistakes can reduce reimbursement now.
AI-Based Claim Review Systems Are Now Common
Insurance payers now use automated tools to review psychiatry claims. These AI-empowered tools review errors and patterns across large volumes of data more efficiently.
These systems check:
- note similarity,
- modifier consistency,
- psychotherapy timing,
- copy-paste behavior,
- and E&M time overlap.
They can detect patterns across hundreds of claims at once. A small documentation mistake used to affect a few claims. Now it exposes an entire provider panel to audit risk.
The 6 Biggest Documentation Risks in Psychiatry Billing in 2026
These are the 6 most common documentation mistakes that cause denials and audits in psychiatric practices. The good news is that each one can be avoided.
1. Incorrect Telehealth Modifiers
Telehealth claims are getting denied in 2026 because many practices are still using outdated modifiers.
- Modifier 95 is used for audio-video telehealth sessions.
- Modifier -93 is used for audio-only sessions.
- Note must explain why video was not used.
Traditional Medicare is not accepting the legacy GT modifier for standard telehealth billing anymore. When you use the modifier that does not match the type of session documented in the note, the claim can be denied automatically.
2. No Start/Stop Times in Session Notes
Psychotherapy CPT codes such as:
- 90832
- 90834
- 90837
depend on documented session duration. The #1 denial trigger in psychiatry is missing exact start and stop times. If a documentation says:
“45-minute psychotherapy session”
It will be insufficient without exact start and stop times recorded in the note.
According to AAPC (2026):
“Psychotherapy time should always reflect the exact duration of the therapeutic interaction… Phrases such as ‘approximately 45 minutes’ create ambiguity and can raise red flags during audits.”
3. Weak Medical Necessity Documentation
In your notes the patient’s symptoms should connect to the DSM-5 diagnosis and the specific intervention you used for that. If you write vague language like;
“patient reports doing better”
It does not clear why the treatment is medically necessary.
Your documentation should clearly show:
- current symptoms
- functional impairment
- diagnosis relevance
- why the chosen intervention is clinically necessary
4. E&M and Psychotherapy Time Overlap
Combined billing scenarios such as:
- 99214 + 90833
- 99213 + 90836
continue to create audit exposure. When both codes are billed together, psychotherapy time cannot also be counted toward E&M time.
Sometimes providers unintentionally count the same time twice when they are documenting both medication management and psychotherapy in one session. Insurance review systems can now catch these mistakes very quickly.
5. Incorrect Place-of-Service Coding
Place-of-service coding errors are common in tele-mental health billing.
- POS 10 means the patient is at home.
- POS 02 applies when the patient is located at another telehealth site
If you choose the wrong POS code, it can change reimbursement rates and trigger automatic review flags.
6. Missing SUD Consent Under New 42 CFR Part 2
In 2026, the rules are updated. Now patients receiving substance use disorder (SUD) treatment must have updated consent documentation.
If the consent form is missing or outdated, practices can face:
- denials
- audit findings
- regulatory compliance issues
This risk increased significantly after the 2026 enforcement changes.
Table: What Payers Are Auditing in 2026
| Documentation Risk | CPT Code Affected | Consequence | Risk Level |
| Missing start/stop session times | 90832, 90834, 90837 | Automatic denial; no appeal path without documentation correction | Critical |
| Wrong telehealth modifier (GT instead of 95) | All telehealth codes | Denial or reduced payment; Medicare won’t accept GT for traditional fee-for-service | Critical |
| Audio-only without documented reason for no video | Modifier -93 claims | Denial; audio-only requires explicit documentation of why video was not used | Critical |
| E&M + psychotherapy time double-counted | 99213/99214 + 90833/90836/90838 | Overpayment recovery; audit trigger; potential fraud allegation | Critical |
| 90791 vs 90792 confusion | 90791, 90792 | Denial or underpayment; 90792 requires medical services component | High |
| Vague medical necessity language | All psychotherapy codes | Retroactive denial on audit; clawback demand | High |
| Missing 42 CFR Part 2 SUD consent (post Feb 16) | SUD-related claims | Denial; HIPAA compliance risk; potential regulatory action | High |
| Incorrect POS code for telehealth | All telehealth claims | Wrong reimbursement rate; potential recovery demand | High |
| Copy-paste notes with no individualized content | All codes | Major audit flag; payer may deny entire episode of care | Critical |
| Group therapy without attendance/participation notes | 90853 | Denial if individual member notes are absent or generic | Moderate |
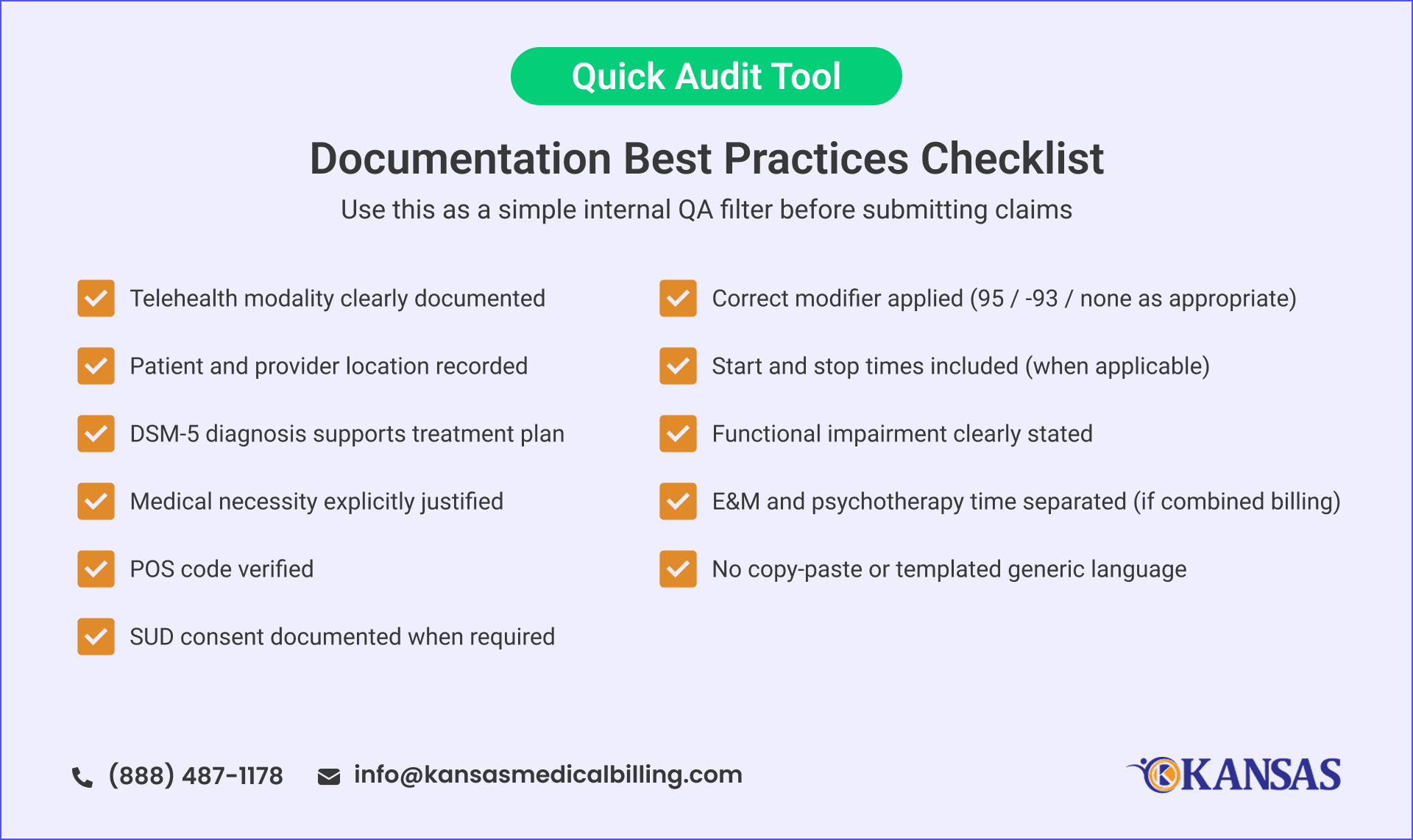
How to Reduce Psychiatry Billing Denials in 2026
The cause of most psychiatry billing denials is not clinical quality issues. They are caused by missing, inconsistent, or non-defensible documentation structure.
To reduce denial risk, practices need to move from narrative-style notes to audit-ready structured documentation. This system connects clinical reasoning to billing.
Here are what you can do:
1. Standardize Telehealth Documentation Templates
Your telehealth note should include:
- Modality (video vs audio-only)
- Reason for audio-only (if applicable)
- Patient location
- Provider location
- Correct modifier (95 or -93)
- Place-of-service (POS 10 or POS 02)
This reduces the common mismatch errors.
2. Make Time Documentation Non-Negotiable
For psychotherapy and time-based services, always document:
- Start time
- Stop time
- Total duration
- Service type (med management vs psychotherapy vs combined)
Avoid estimated or rounded durations unless it is allowed by payer policy.
3. Strengthen Medical Necessity Language
Your notes should clearly connect:
Symptoms → Functional impact → DSM-5 diagnosis → Intervention used
Instead of vague phrases like, use clinical language such as:
4. Separate E&M and Psychotherapy Time Clearly
When billing combined services:
- Clearly distinguish medication management time from psychotherapy time
- Avoid overlapping descriptions
- Make sure the psychotherapy time is independently mentioned
This is one of the most common audit recovery triggers in outpatient psychiatry.
5. Audit Place-of-Service Accuracy
Telehealth POS errors are simple but they are very costly. Build a verification step into your workflow to confirm:
- POS matches patient location
- POS aligns with telehealth modality
- Modifier and POS are consistent
Even small inconsistencies can cause automated claim rejection.
6. Maintain Updated 42 CFR Part 2 Consent Files
With the 2026 enforcement update:
- Consent must explicitly cover treatment, payment, and healthcare operations
- SUD documentation must be current and accessible
- Missing or outdated consent can result in immediate denial
Make sure to follow all these steps for compliance-critical documentation.
Stop Losing Revenue to Preventable Documentation Errors
Psychiatry billing is no longer just about submitting claims. It’s about submitting audit-proof documentation that survives AI-based payer review systems. Small gaps in telehealth coding, time tracking, or medical necessity language can now lead to denials.
If you are not sure whether your documentation meets 2026 payer standards, Kansas Medical Billing can help.
Our psychiatric billing specialists audit your current documentation against 2026 payer requirements. and fix the gaps before they become denials.
No obligation. We review up to 20 charts and identify your top documentation risks.
Frequently Asked Questions
1. What makes psychiatric notes more audit-sensitive today?
AI review systems now scan large claim sets for consistency, making even small documentation gaps easier to detect across multiple visits.
2. Why do behavioral health claims need stricter structure now?
Because subjective improvements alone are no longer sufficient; payers expect clearly traceable clinical reasoning in every note.
3. How do payers evaluate consistency across sessions?
They compare documentation patterns over time to identify repetition, missing variation, or unsupported clinical progression.
4. What role does clinical reasoning play in billing approval?
It demonstrates why a specific treatment approach was chosen, linking clinical decisions to measurable patient needs.
5. Why are psychiatry practices facing more compliance pressure?
Because telehealth growth and automated claim screening have increased the volume and precision of billing reviews.



